Strongyloidiasis
Strongyloidiasis
Section Contents
Key Points
- Strongyloidiasis is a parasitic infection caused by the nematode Strongyloides stercoralis.
- Infection occurs when infective larvae, present in fecally contaminated soil, penetrate the intact skin.
- The life cycle is very complex and consists of two separates phases: a free-living phase and a parasitic phase.
- S. stercoralis can complete its entire life cycle inside the human host (autoinfection), allowing it to persist for decades.
- Strongyloides infection has an acute and a chronic phase. Further, in those taking corticosteroids, co-infected with HTLV-1 and/or other immunosuppressive conditions, a hyperinfection syndrome can occur.
- Ivermectin is the drug of choice for treatment.
Background & Epidemiology
Strongyloidiasis is a parasitic infection caused by the soil-transmitted helminth Strongyloides stercoralis. Because of its uniqueness, we gave it a separate lesson! Other species (S. fuelleborni, S. fuellerborni kellyi) will not be discussed in this module. S. stercoralis has a worldwide distribution, but it is primarily seen through tropical and subtropical areas.
Although the exact prevalence is unclear, an estimated 30-100 million people are infected worldwide. Infection by S. stercoralis occurs by skin penetration of infectious larvae present in soil, which occurs frequently while walking barefoot in endemic areas.
Transmission & Life cycle
It involves two separate phases, a free-living (in the environment) and a parasitic phase (in the human). Click below to learn more on each:

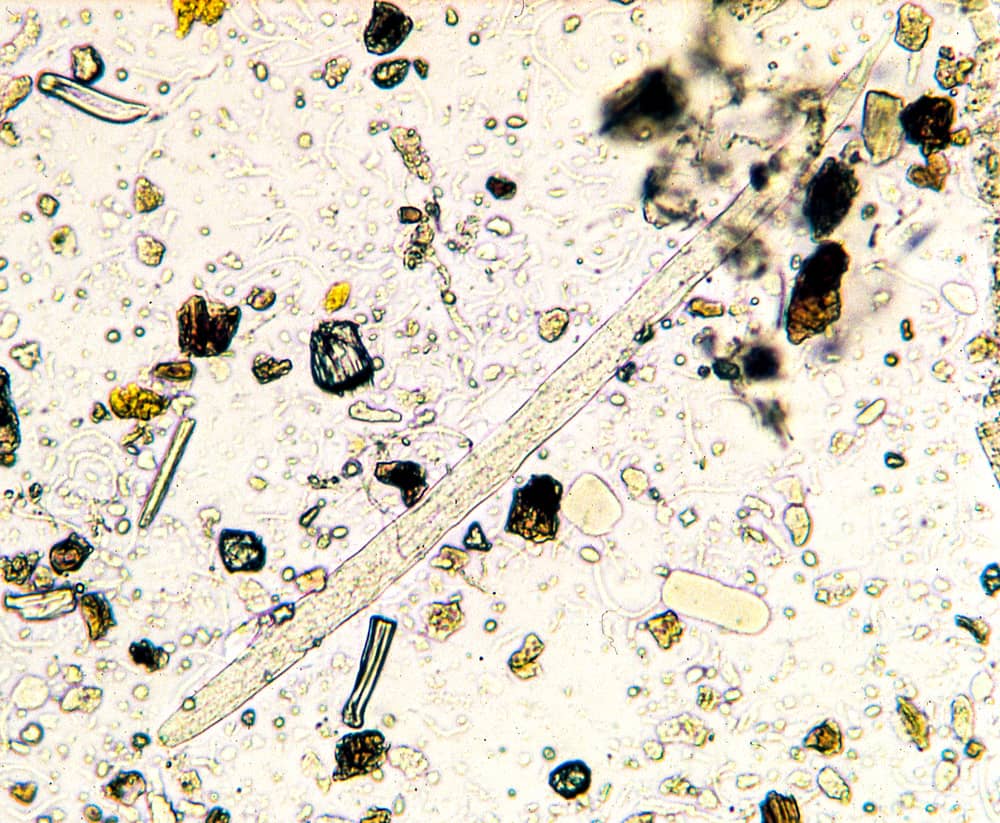
Figure 1. Strongyloides larva

Figure 2. Life cycle of Strongyloides stercoralis
Pathogenesis & Clinical Presentation
During the parasitic phase, Strongyloides can have different presentations at each phase of the life cycle:
Answer
Löeffler's syndrome is a transient hypersensitivity reaction to the larval cuticle during the L3 to L4 molting process. Once the cuticle disappears, the respiratory symptoms go away and appear in other body sites where the larva is present.
Diagnosis
As with all diseases, diagnosis starts with a clinical suspicion in the right epidemiological context (ask yourself: What is the presentation? Who is the host?). Clinical and epidemiological diagnosis is supported with various diagnostic modalities. In the case of Strongyloides, diagnosis is challenging because there is no gold standard test, but available diagnostics include:
- Acute infection:
- Stool microscopy (direct smear): sensitivity is low, and requires serial testing. Might be more helpful among individuals with high parasitic burden (e.g., AIDS). Concentration techniques (i.e., Baermann concentration) are preferred, but are not widely available.
- Different from other helminthiasis, stool examination will show
rhabditiform larvae (L1)! NOT eggs. L3 larvae are rarely seen because
they re-penetrate the mucosa before being released with stool.
- Different from other helminthiasis, stool examination will show
- Agar plate culture: after placing a stool sample in an agar plate, larvae can
carry enteric bacteria through the plate, showing centrifugal tracks. Modifications using cellophane paper are available, click here to read more! - PCR: highly sensitive and specific, but not widely available.
- Serology: can be initially negative. Does not differentiate between previous or past infection. Useful in non-endemic areas.

Figure 3. Strongyloides larvae in stool
- Stool microscopy (direct smear): sensitivity is low, and requires serial testing. Might be more helpful among individuals with high parasitic burden (e.g., AIDS). Concentration techniques (i.e., Baermann concentration) are preferred, but are not widely available.
- Chronic infection:
- Stool microscopy/PCR: frequently negative, due to the low and inconsistent shedding of larvae released in stool.
- Agar plate: in certain endemic areas, agar plate is considered test of choice during chronic infection. Serial examination can improve sensitivity.
- Serology (ELISA - IgG): sensitivity is high, but can cross react with other helminths. Only shows past exposure. Test of choice during chronic infection in non-endemic areas.
- Hyperinfection & Disseminated syndrome:
- Serology
- Stool & sputum microscopy: because of high burden of migrating larvae, they may be seen in stool AND in sputum! Don't forget to send both!

Treatment
The drug of choice for Strongyloides stercoralis is ivermectin!
- Uncomplicated (acute or chronic) infection: in books you will find that treatment of choice is ivermectin 200 mcg/kg/day for 1-2 days. Certain experts will argue that a single dose 150-200 mcg/kg/d is usually sufficient, but dose might be repeated 14-30 days later if eosinophilia has not improved.
- In immunocompromised individuals, 1-2 doses should be repeated 14 days later.
- Hyperinfection & disseminated syndrome: ivermectin is still the drug of choice, but duration is debated. You should be managing this in consultation with an expert!
- Rectal or parenteral formulation has been used off-label.
- Reduce immunosuppression as possible.
Answer
NUMBER ONE - screen patients at risk with serology before starting immunosuppressive therapy or those with HTLV-1 infection.
NUMBER TWO - Ivermectin is contraindicated in patients with Loa Loa co-infection (screen based on epidemiological risk!). More on this in Filarial Nematodes.
Prevention
- Avoid contaminating soil with human stool (e.g., proper disposal of human waste).
- Avoid coming in contact with contaminated soil (e.g., wearing shoes in endemic areas).
- Screen and treat patients at risk! (as noted in management pearls).
NOTE: high-risk occupations in endemic areas include those involved in agriculture, gardening, septic tank cleaners, among others.
Assessment: Did I Get It? (DIG IT)
DIG ITs are online modules designed to reinforce key learning points for you! Please choose the best answer, then check all of the answer choices for more learning pearls
Other Media Resources (Optional)
References
This lesson was last updated September 8 2025