Zoonotic Nematodes
Zoonotic Nematodes
Editor: Jill Weatherhead
Section Contents
- Toxocariasis
- Cutaneous larva migrans
- Assessment: Did I Get It? (DIG-IT)
- References
Toxocariasis
Key Points
- Toxocara is a zoonotic nematode acquired from ingesting eggs from soil contaminated with feces of dogs and cats.
- Humans are accidental hosts and larvae migrate through tissues (e.g., liver, lungs, brain, eye) without ever molting into adults.
- It is widely distributed and it mainly affects children.
- Toxocariasis can range from asymptomatic infection to visceral or ocular larva migrans.
- Diagnosis is through serology. In the case of ocular disease, a retinal exam is key!
Background & Epidemiology
Toxocariasis is a parasitic disease caused by the ascarid nematode of the genus Toxocara. Adult worms live in the intestines of dogs (T. canis) and cats (T. cati). Humans - who are accidental hosts - get infected when they ingest embryonated eggs present in soil contaminated with feces from dogs and/or cats (mainly puppies/kittens).
In humans, toxocariasis can produce a wide range of clinical manifestations from asymptomatic infection with/without eosinophilia to visceral and ocular larva migrans syndromes (more on this in Clinical Presentation).
Toxocariasis occurs mainly in children, because they are more prone to eat dirt. Occasionally, adults can get infected. Toxocariasis is widely distributed among places where soil is contaminated with feces of dogs/cats (i.e. sandpits in public parks, playgrounds, beaches) - this can be particularly prevalent among communities where stray dogs and cats are widespread.

Figure 1. Stray dog and other animals in rural community in Guarico, Venezuela
Life Cycle

Figure 1. Life cycle of toxocariasis
Clinical Presentation
Incubation period is variable but ranges from weeks to months. The clinical spectrum of toxocariasis ranges from asymptomatic infection with/without eosinophilia to visceral and ocular larva migrans.
- Covert or occult toxocariasis → occurs when symptoms & eosinophilia are absent or mild, but serology is positive.
- Visceral toxocariasis or visceral larva migrans (VLM) → occurs when multiple larvae migrate through tissues leading to a higher inflammatory response. It can cause fever, hepatosplenomegaly, bronchospasm, eosinophilic pneumonia, and urticaria. Less commonly, CNS invasion (i.e., encephalopathy, eosinophilic meningitis, seizures, neuropsychiatric disorders) occurs.
-
- Demographics: it's more common in pre-school children (usually <5 years).
- Laboratories: HIGH eosinophil count, HIGH immunoglobulin (IgM/IgG/IgE) levels. Elevated isohemagglutinin levels can support the diagnosis.
- Imaging: multiple hepatic and pulmonary nodules can be seen on abdominal/chest imaging.
- Prognosis: disease is typically self-limited in 1-2 years, but can be fatal if invasion of the CNS occurs.
Note: When you see multiple ill-defined liver lesions in a patient with eosinophilia, think of Toxocara o Fasciola! -
- Ocular toxocariasis or ocular larva migrans (OLM) → occurs when an isolated larva erratically migrates to the eye. Larva get retained in the posterior pole (more commonly in the periphery) and lead to granulomas that drag the retina and create a distortion of the macula, and can cause leukocoria, blurry vision, floaters, and strabismus! Be aware that these granulomas may resemble retinoblastoma!!!
-
- Demographics: it's more common in older children (5-10 years) and adolescents;
- Laboratories: because inflammatory response is milder, eosinophilia is VARIABLE;
- Prognosis: if untreated, it can lead to unilateral chorioretinitis, retinal detachment, and permanent vision loss.
Note: Patients with toxocariasis tend to have only ONE syndrome. Either they have VLM or OLM, but rarely both! -

Figure 2. Ocular larva migrans
Diagnosis
As with all diseases, diagnosis starts with a clinical suspicion in the right epidemiological context (What is the presentation? Who is the host?). Here is a quick review for you:
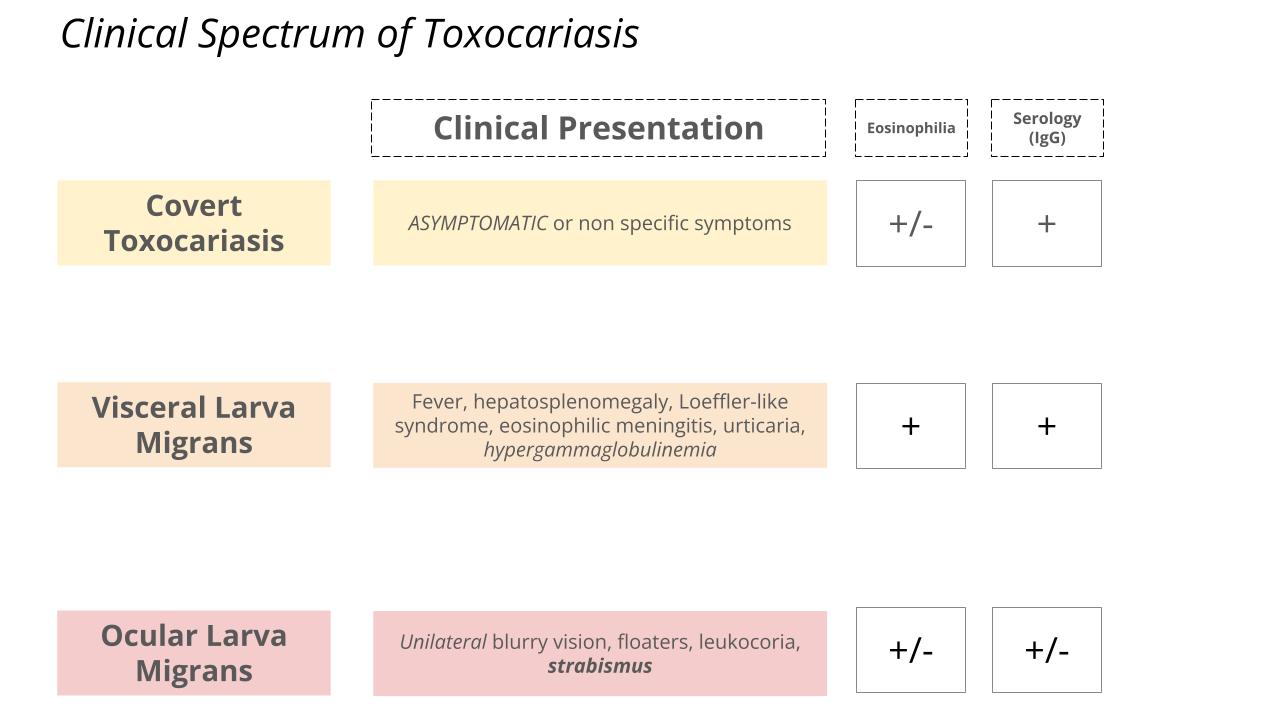
Figure 3. Clinical spectrum of toxocariasis
Suspect toxocariasis in children with unexplained eosinophilia & hypergammaglobulinemia, fever, organomegaly, and Loeffler-like syndromes OR in those with unilateral posterior segment granuloma! Particularly those with pica, and exposure to domestic pets (i.e., puppies, kittens) in recent years. Definitive diagnosis will depend on the following modalities:
Treatment & Management
- Covert/Occult toxocariasis → treatment can be considered but may not be necessary.
- VLM → Albendazole is the drug of choice (PLUS steroids in severe cases and/or neurologic involvement). Although most literature recommends albendazole 400 mg BID for 5 days, some authors recommend treatment for at least 3-4 weeks based on the clinical scenario.
- OLM → Corticosteroids (topical/systemic) are used to help with the inflammation (if present). Albendazole has variable efficacy; but if used, steroids must be started before!
- Please call an ophthalmologist!
- Surgery may be needed if there are complications such as retinal detachment, or macular fibrosis, etc.
Prevention
At the animal level:
- Discuss deworming your pets with the vet.
- Clean up after dogs and cats who defecate in soil to avoid embryonation of eggs.
- Control of stray dogs and cats.
- Inform pet owners of risks of toxocariasis in animals.
At the human level:
- In possible, avoid pica.
- Enforce hand hygiene, especially in children after playing in sandpits & parks.
- Inform parents of risks of toxocariasis in children.
Cutaneous larva migrans
Key Points
- Cutaneous larva migrans is the clinical syndrome in humans caused by larval stages of hookworms of dogs and cats (Ancylostoma caninum & A. braziliense).
- Larvae penetrate unbroken skin and form a highly pruritic, serpiginous lesion as it migrates through the epidermis.
- Diagnosis is made clinically.
- Treatment is with Ivermectin or Albendazole.
Background, Epidemiology & Life Cycle
Cutaneous larva migrans (CLM) is the clinical syndrome in humans caused by larval stages of hookworms of dogs and cats (Ancylostoma caninum & A. braziliense). They live in the intestine of cats and dogs and pass eggs that hatch and release larvae in soil. Larvae become infectious in 1-2 weeks and can survive for several weeks in the appropriate environment. Humans acquire CLM through skin contact with the infectious larva, which classically occurs by walking barefooted (e.g., beaches, sandy/moist soil).
Human infection occurs when L3 larva penetrates the unbroken skin. The larva is unable to penetrate deeper skin layers and migrate erratically though the epidermis. Humans are accidental hosts and thus zoonotic hookworm larvae are unable to complete its life cycle.
These larvae are especially common in tropical and subtropical areas (e.g., Southeast Asia and the Caribbean), where dogs and cats are permitted to wander the beach and freely defecate. In the United States, CLM is particularly prevalent along the Gulf of the Atlantic coasts of Florida and the Carolinas.
 Clinical Presentation & Diagnosis
Clinical Presentation & Diagnosis
 Clinical Presentation & Diagnosis
Clinical Presentation & DiagnosisAfter penetrating the unbroken skin, a papule forms at the inoculation site within a few hours. Over several days, a serpiginous, highly pruritic track (known as “creeping eruption”) forms as the larva migrates through the epidermis. Larva advances a few centimeters a day, and typically dies within 10 days (although some can last longer). Lesions are more common in feet, but can occur in other points of contact with soil (e.g., buttocks, abdomen). Image to the right shows CLM (photo courtesy of Gala Godoy Brewer, MD). Secondary bacterial infections caused by scratching can occur. Diagnosis is made clinically.
All of the larva migrans syndromes sound similar and can be confusing! Here is a review for you!
| Cutaneous larva migrans | Visceral larva migrans | Ocular larva migrans | Larva currens | |
|---|---|---|---|---|
| Pathogen | Ancylostoma braziliense | Toxocara canis/cati | Toxocara canis/cati | Strongyloides stercoralis |
| Clinical presentation | Serpiginous, pruritic lesions “creeping eruption” | Fever, organomegaly, Eosinophilic pneumonia/wheeze, urticaria | Posterior segment granuloma, uveitis, endophthalmitis | Serpiginous, pruritic, lesions (rapid progression) |
| Diagnosis | Clinical | Clinical + Serology | Clinical + Serology | Clinical + Serology + Stool and/or BAL |
| Treatment | Albendazole or Ivermectin | Albendazole +/- Steroids | Steroids +/- Albendazole +/- Surgery | Ivermectin |
Table 1. Summary of CLM, VLM, OLM, and larva currens
Treatment & Management
Single dose ivermectin OR albendazole 400 mg BID for 3-7 days.
Assessment: Did I Get It? (DIG-IT)
Assessment: Did I Get It? (DIG IT)
DIG ITs are online modules designed to reinforce key learning points for you! Please choose the best answer, then check all of the answer choices for more learning pearls
References
This lesson was last updated May 5 2025