Serologic testing for IgM and IgG is the preferred method of diagnosis for both acute and remote infections. A variety of assays are available for testing, but the serological standard is an enzyme-linked immunosorbent assay (EIA). At the time of symptom onset, most patients have detectable IgM and IgG antibodies. RT qPCR is also great, and it can be detectable several weeks prior to and after the resolution of symptoms.
Hantavirus and Avian Influenza
Hantavirus and Avian Influenza
Maxine F. Chang, MD
Department of Medicine, Division of Infectious Diseases, Columbia University Irving Medical Center, New York, New York, USA
Author: Maxine F. Chan
Shauna H. Gunaratne, MD, MPH, CTropMed
Department of Medicine, Division of Infectious Diseases, Columbia University Irving Medical Center, New York, New York, USA
Editor (hantavirus): Shauna H. Gunaratne
Prof. Yuen Kwok Yung, MD
Henry Fok Professor in Infectious Diseases, Chair of Infectious Diseases, The University of Hong Kong, Hong Kong
Editor (avian influenza): Professor Yuen Kwok Yung
Section Contents
- Hantavirus
- Key aspects
- Background
- Epidemiology & Transmission
- Clinical Presentation
- Diagnosis
- Treatment
- Prevention
- Avian Influenza
- Key aspects
- Background
- Epidemiology & Transmission
- Clinical Presentation
- Diagnosis
- Treatment
- Prognosis
- Prevention
- References
Hi there! In this lesson, we’ll talk about two viruses that have been making headlines lately: hantavirus and avian influenza. They’re just two members of a much larger group of viruses with pandemic potential (including Ebola, Mpox, and other coronaviruses), some of which will be covered in separate lessons. Together, hantavirus and avian influenza offer a timely and interesting look at how viruses emerge, spread, and capture public attention. Enjoy!
Hantavirus
Key aspects
- Hantaviruses are spread primarily via rodents, through their droppings, urine, saliva, and more rarely, via bites/scratches
- The two clinical syndromes associated with hantaviruses are hemorrhagic fever with renal syndrome (HFRS), endemic to Asia and Europe, and hantavirus cardiopulmonary syndrome (HCPS), endemic to the Americas
- Clinical outcomes are highly correlated with early recognition and diagnosis, and treatment is supportive
Background
Hantaviruses are part of the genus Orthohantavirus, a group of enveloped, single stranded RNA viruses. They are a zoonotic infection that is spread primarily through rodents.
Hantavirus infections are associated with two clinical syndromes (this is high yield!):
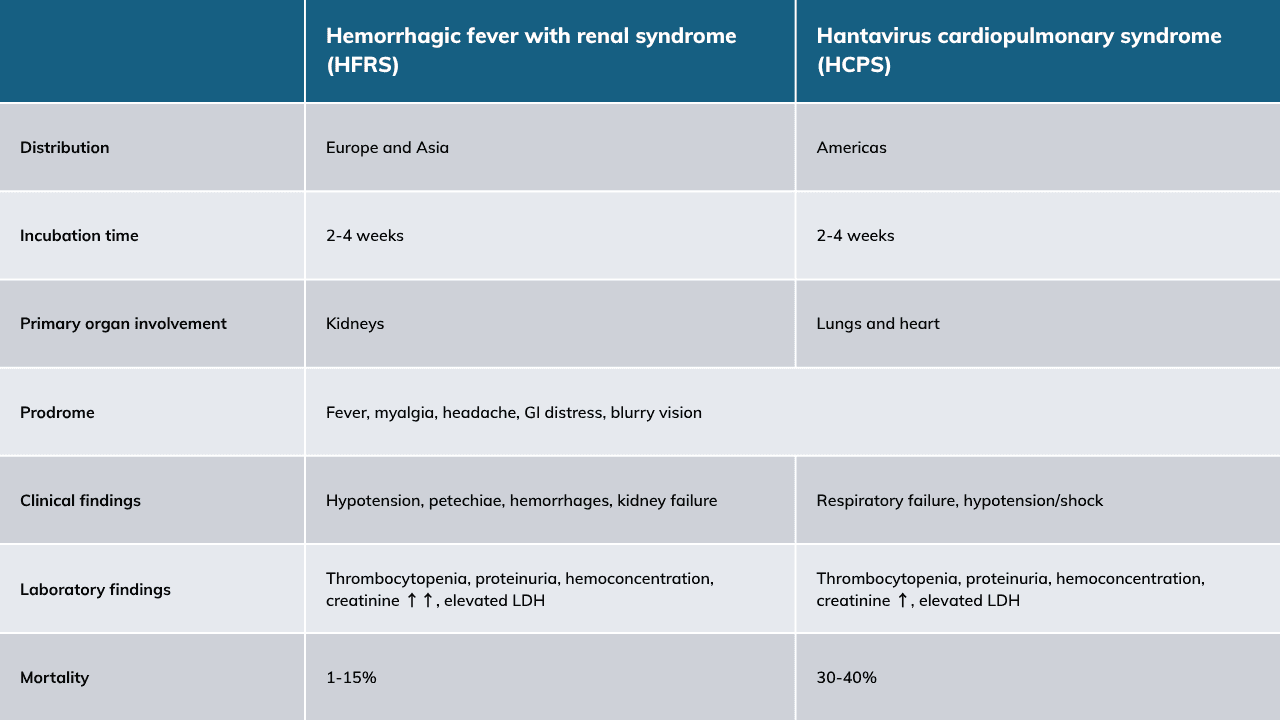
- Hemorrhagic fever with renal syndrome (HFRS), caused by viruses of the Old World (Europe and Asia)
- Hantavirus cardiopulmonary syndrome (HCPS), caused by hantaviruses of the New World (the Americas).
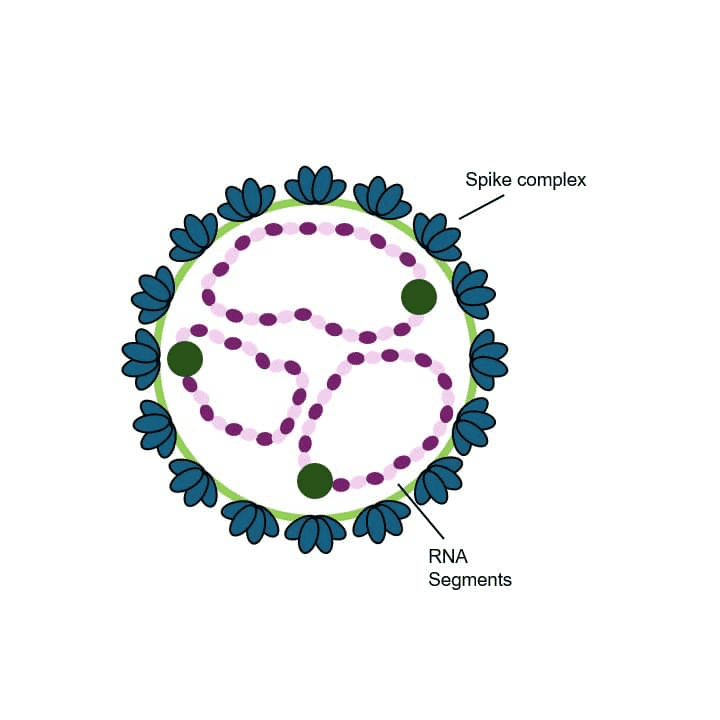
Figure 1. Hantavirus structure
Epidemiology & Transmission
Rodents are the main reservoirs for hantaviruses and are associated with a single species of rodent, though other animals, including bats, moles, reptiles, and even fish can carry the infection. Seroprevalence of hantavirus antibodies in rodents ranges between 1-20%, and these animals typically have active, persistent infection.
There are over 40 species of hantavirus in nature, with approximately 22 species pathogenic to humans. In Europe and Asia, the majority of HFRS infections are carried by field mice and rats. Of those viruses that cause HCPS in the Americas, the deer mouse is the major reservoir of the Sin Nombre virus (SNV), the most important cause of this syndrome in North America. The most common viruses and their reservoir hosts, along with countries where infections have been reported, are tabulated below.
The highest incidence of HFPS infections occurs in China, with Hantaan and Seoul virus as the main strains implicated in infection. In North America, significant outbreaks have occurred in New Mexico, California, Arizona, and Colorado, caused by the Sin Nombre virus.

Figure 2. Approximate distributions of Hantaviruses that cause human disease
Transmission: Hantaviruses are transmitted via inhalation of aerosolized virus in rodent feces, saliva, and urine. Rarely, infection can also be transmitted via animal bites or scratches. Person-to-person transmission has also been reported but is not a major mode of spread.
NOTE: Andes virus remains the only hantavirus known to spread between people. The 2026 outbreak of Andes hantavirus among passengers and crew aboard the cruise ship MV Hondius provided clear evidence of limited human-to-human transmission (with 11 cases total), occurring after an initial rodent-derived exposure.
Clinical Presentation
As mentioned above, hantavirus infections can be divided into two clinical syndromes: hemorrhagic fever with renal syndrome (HFRS), typically in Europe and Asia, and hantavirus cardiopulmonary syndrome (HCPS), typically in the Americas. While different clinical entities, both infections share similar prodromes and cause intense inflammatory responses.
Incubation time of each is typically ~2-3 weeks (though can be up to 6 weeks, yikes!), with a prodrome consisting of high fevers, headaches, myalgias, abdominal, and back pain.
Laboratories: The first abnormality is typically thrombocytopenia, which can occur during the prodromal phase. Other laboratory abnormalities include proteinuria, elevated creatinine, and increased LDH, typically seen during the cardiopulmonary phase.
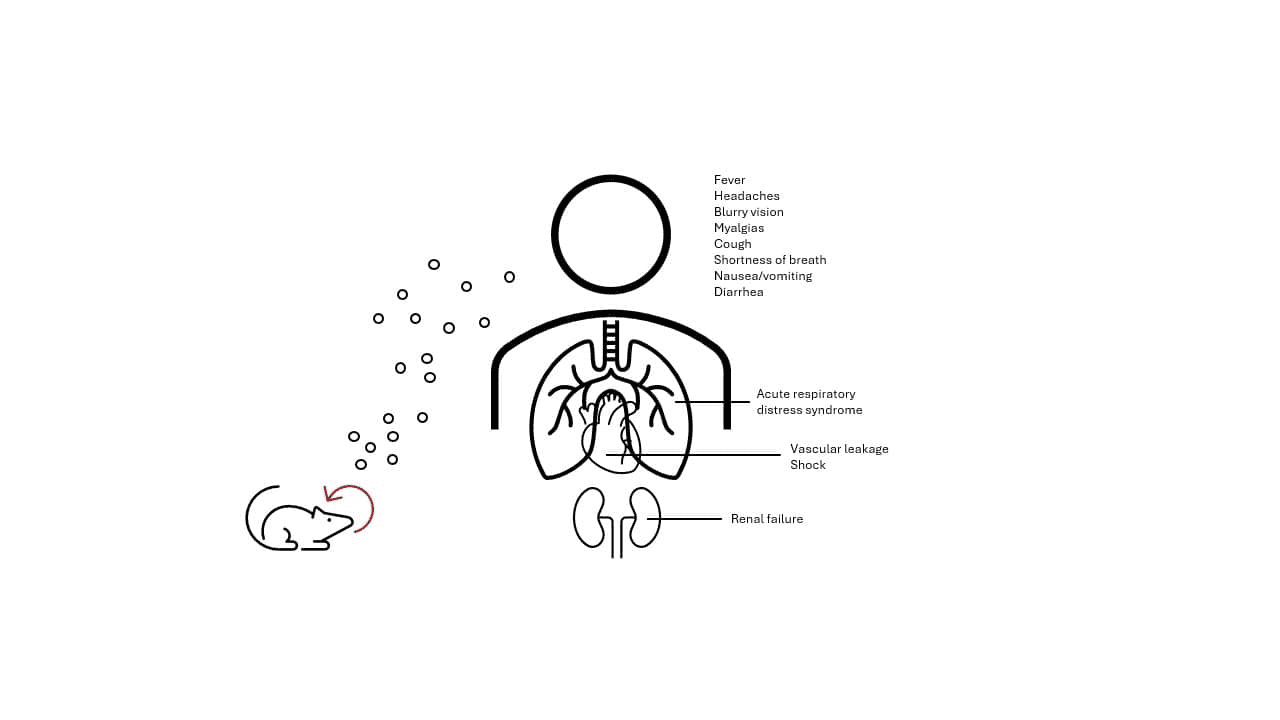
Figure 3. Transmission and symptoms
Diagnosis
As ever, diagnosis of HFRS and HCPS requires a high degree of suspicion, especially as early prodromal symptoms are indistinguishable from other common viral illnesses. Infection should be considered in patients who have had travel to endemic regions, and present with prodromal symptoms of fever, headache, myalgias, and gastrointestinal distress. Notably, typical features associated with upper respiratory viruses (with the exception of cough), such as pharyngitis, rhinorrhea, are absent! CDC clinical descriptions for HCPS emphasize a characteristic pattern on complete blood count (CBC) that supports the diagnosis, with typical findings including hemoconcentration, leukocytosis with a leftward shift, increased immunoblasts, lack of significant toxic changes in neutrophils, and thrombocytopenia.
What is the diagnostic method of choice for hantaviruses?
Answer:
Treatment
HCPS: To date, there are no effective antiviral treatments for the management of HCPS, and treatment is supportive. Given the high risk of rapid cardiopulmonary collapse, patients should be transferred to centers with critical care units with access to extracorporeal membrane oxygenation (ECMO)!!! [Think cardio-ECMO]
HFRS: Management of the associated renal failure includes close electrolyte, blood pressure, and fluid status monitoring. Ribavarin has shown benefit in reducing mortality and improving outcomes (decreased progression to renal failure and hemorrhage) in some forms of HFRS when given early in the disease course. [Think Renal-Ribavirin]
PROGNOSIS: Mortality is higher in HCPS (approximately 30-40%). Convalescence from severe infections can take weeks, and chronic sequelae including persistent fatigue, myalgias, shortness of breath, and renal damage have been reported.
Prevention
Prevention → limiting contact with rodents. Special attention to those at high risk of exposure (e.g., rodent exterminator) severe infection, including young children, pregnant women, or immunocompromised individuals!
Pest control → rodent pest control in inhabited spaces is important for preventing the spread of infection. Buildings should be inspected for potential rodent entry sites, which should then be sealed, and areas of heavy brush and debris (ideal nesting sites) should be cleared. If nests are discovered, to reduce the risk of droppings and urine aerosolization, these should be soaked in a bleach solution prior to cleaning. At a minimum, rubber or plastic gloves should be used to handle soiled material, though for heavier infestations, respirator use may also be needed.
Vaccines → There are no Food and Drug Administration (FDA) or European Medicines Agency (EMA) approved vaccines currently on the market. However, in Korea and China, an inactivated vaccine has been developed to prevent HFRS specifically caused by the Seoul and Hantaan viruses, and may be administered to individuals at high risk of exposure.
Avian Influenza
Key aspects
- Avian influenza (aka “bird flu”) is caused by an influenza A virus that typically affects birds, but can spread to humans
- Seasonal influenza in humans is caused by influenza A subtypes H1 and H3, while the most common avian subtypes are H5 and H7
- The spectrum of infection is broad, but is typically characterized by fever and severe lower respiratory symptoms
- Diagnosis requires a high degree of suspicion, and influenza A subtyping is helpful
- Early treatment with oseltamivir, along with robust infection control measures, is recommended
Background
Avian influenza is caused by an influenza A virus that infects both wild (gulls, ducks, shorebirds) and domestic poultry (chickens, ducks, geese). Influenza A viruses are categorized into subtypes based on their surface proteins, hemagglutinin (H) and neuraminidase (N). There are 18 hemagglutinin subtypes and 11 neuraminidase subtypes found in the avian and mammal reservoirs, and different subtypes affect different species.
Avian influenza structure
In humans, only subtypes H1N1 and H3N2 are currently circulating, and they are responsible for the seasonal flu. In birds, almost every combination of H1-16 and N1-11 has been isolated; however, only five subtypes of influenza A (H5, H6, H7, H9, and H10) have been identified in human infections, with subtypes H5, H7, and H9 being the most common. Mutations in the surface proteins of avian strains of influenza can bind to receptors in the human respiratory tract, allowing the virus to spread to people under the right conditions. Genomic sequence reassortment between different viral subtypes during co-infection with two different influenza viruses can also create new hybrid strains, increasing the risk of interspecies jumping (i.e. from birds to humans).
Epidemiology & Transmission
Avian influenza is endemic in wild bird populations around the word, and subtypes are classified into “high pathogenic avian influenza” and “low pathogenic avian influenza” strains based on how deadly the virus is for chickens in a laboratory setting. Highly pathogenic strains of avian influenza have typically emerged when low pathogenic viruses cross from wild birds to domestic poultry, with subsequent mutations increasing virulence.
The two strains responsible for most avian and human infections are H5N1 and H7N9. The first case of H5N1 in humans was reported in 1997, and between 2003 and 2025, there have been >980 human cases linked to this strain. H7N9 has been responsible for >1560 cases in humans between 2013 and 2025.
Infection is rapidly spread between birds via respiratory secretions and droppings. In Asian countries, this occurs mainly amongst domestic poultry, while in North America and Europe, spread is primarily via migratory birds. Transmission to humans is uncommon, but can happen via inhalation of respiratory drops, or from direct animal or fomite contact. Limited, non-sustained person-to-person spread has been reported, including via vertical transmission, but this is very uncommon. Avian influenza can also spread to other domesticated animals such as dairy cattle and pigs, which can then transmit the virus to humans.

Avian Influenza Epidemiology & Transmission
Clinical Presentation
The incubation period from exposure is typically 3-5 days, though may be up to 10 days. Presentation is highly variable, ranging from asymptomatic to fulminant pneumonitis with multiorgan failure.
Mild infections cause symptoms like those of seasonal influenza, which include fever, conjunctivitis, sore throat, cough, myalgias, malaise, headache, and GI upset. More severe symptoms include shortness of breath and altered mentation.
Death is most commonly caused by complications of respiratory failure, including acute respiratory distress syndrome, pneumonia, and pulmonary hemorrhage.
Diagnosis
A diagnosis of avian influenza should be suspected in individuals with the right symptoms in the right clinical context (relevant exposure to wild birds or domesticated poultry and livestock).
What are the diagnostic tests available for bird flu?
Answer:
Influenza A viruses can generally be diagnosed via antigen tests, which look for pieces of viral proteins), or molecular tests, which look for viral nucleic acids (RNA). For mild infections, nasopharyngeal and throat swabs, +/- conjunctival swabs, placed into a viral transport medium are the specimen of choice. For more severe cases, sputum, endotracheal aspirate, or bronchoalveolar lavage should be considered if available. If you suspect avian influenza (either from their exposure history or the severity of their infection), a molecular test with the ability to determine viral subtypes (ie ability to identify the specific hemagglutinin) is important, to differentiate their virus from seasonal influenza.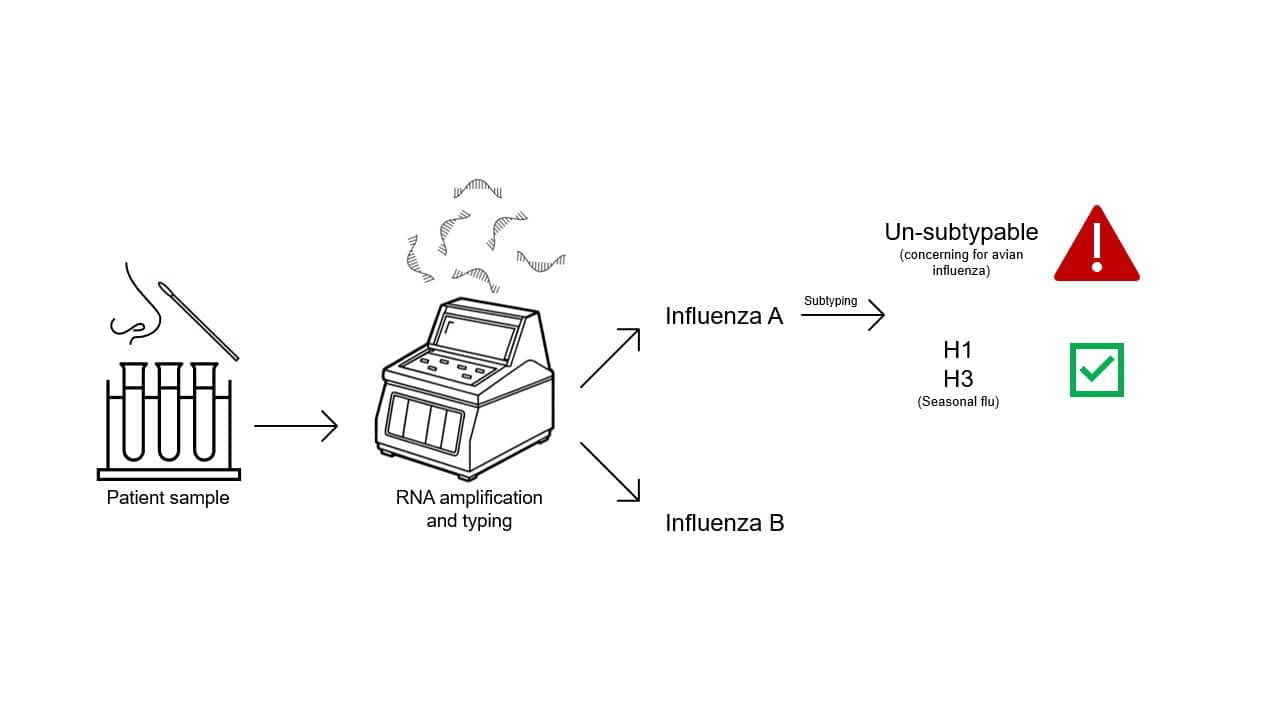
Treatment
Treatment is a combination of antiviral therapy and supportive measures. All patients confirmed or suspected to have avian influenza should receive antiviral treatment. Antiviral options/strategies overlap with those of seasonal flu, though it is still recommended even if a diagnosis is made >48 hours after symptoms start.
Antiviral therapies:
- Oseltamivir* – an oral medication, the first line treatment, duration is uncertain, but usually at least 10 days.
- Peramivir* – an IV medication for patients who cannot take PO
- Zanamivir – an IV medication, used when other antivirals are not available or cannot be administered; inhaled formulations not recommended
* Of note, resistance to these medications can emerge during treatment, and a rebounding viral load may be an indicator
Mild symptoms can be treated with antipyretics, analgesics, mucolytics, cough suppressants, and other over-the-counter cold/flu remedies. Patients with severe illness should receive inpatient management to receive additional supportive care, which in the case of multiorgan failure, may necessitate ventilation, dialysis, and fluid replacement.
Prognosis
As avian influenza is uncommon and because usually only the more severe cases come to medical attention, data on long term outcomes is scarce. Among hospitalized patients, mortality rates for H5N1 range upwards of 30%. Post infection, patients may develop chronic lung scarring, bronchiectasis, pleural thickening, and pulmonary fibrosis.
Prevention
The pillar strategies for avian influenza prevention are similar to those implemented for the seasonal flu.
Infection control
- In health care settings, providers should follow contact (including eye protection), and airborne precautions, and patients should be housed in a negative pressure room
- Domestic poultry flocks that are infected are typically quarantined and/or culled to prevent spread
- Contact with dairy cattle in affected geographical regions should be avoided, and it is recommended that milk products should be pasteurized before consumption
- The general public should avoid contact with infected or dead animals, or other spaces contaminated with animal waste or byproducts
Post-exposure prophylaxis
- Recommended for people with close unprotected contact to an infected person or their secretions
- Recommended for people with close unprotected contact (handling, slaughter, care) of sick/dead birds or animals with confirmed infection
- Prophylaxis should begin as soon as possible, and ideally within 48 hours of the exposure
- Oseltamivir is the preferred agent, with a treatment duration between 5-10 days, depending on the type of exposure
Vaccines
- No avian influenza specific vaccines marketed for current use, but several pre-pandemic vaccines have been developed and authorized for use
- In the event of a pandemic, this would allow for rapid approval and modification for pandemic-specific strains of the virus.
References
a) Hantavirus
- Vial PA, Ferrés M, Vial C, et al. Hantavirus in humans: a review of clinical aspects and management. Lancet Infect Dis. 2023;23(9):e371-e382. doi:10.1016/S1473-3099(23)00128-7
- CDC. “About Hantavirus.” Hantavirus, 13 May 2024, www.cdc.gov/hantavirus/about/index.html.
- Munir N, Jahangeer M, Hussain S, et al. Hantavirus diseases pathophysiology, their diagnostic strategies and therapeutic approaches: A review. Clin Exp Pharmacol Physiol. 2021;48(1):20-34. doi:10.1111/1440-1681.13403
- Andes hantavirus outbreak on a cruise ship, 2026. New England Journal of Medicine. 2026 May 20; doi:10.1056/nejmc2606496
- Huggins JW, Hsiang CM, Cosgriff TM, Guang MY, Smith JI, Wu ZO, et al. Prospective, double-blind, concurrent, placebo-controlled clinical trial of intravenous ribavirin therapy of hemorrhagic fever with renal syndrome. J Infect Dis. 1991 Dec;164(6):1119-27. doi:10.1093/infdis/164.6.1119.
- Severson WE, Schmaljohn CS, Javadian A, Jonsson CB. Ribavirin causes error catastrophe during Hantaan virus replication. J Virol. 2003 Apr;77(9):481-8. PMID:17060520.
- Kim YK, Lee JW, Baek LJ, Song KJ, Kim SH, Park SC, et al. Experience with intravenous ribavirin in the treatment of hemorrhagic fever with renal syndrome in Korea. Antiviral Res. 2009 Jan;81(1):68-76. doi:10.1016/j.antiviral.2008.09.007.
- Koster F, Foucar K, Hjelle B, Scott A, Chong YY, Larson R, McCabe M. Rapid presumptive diagnosis of hantavirus cardiopulmonary syndrome by peripheral blood smear review. Am J Clin Pathol. 2001;116(5):665-672.
b) Avian Influenza
- US Department of Agriculture. Avian influenza fact sheet. Accessed January 2026. https://www.usda.gov
- Centers for Disease Control and Prevention. Types of influenza viruses. Updated periodically. Accessed January 2026. https://www.cdc.gov/flu/about/viruses/types.htm
- Centers for Disease Control and Prevention. Avian influenza type A (bird flu). Updated periodically. Accessed January 2026. https://www.cdc.gov/flu/avianflu/index.htm
- American Ornithological Society. Highly pathogenic avian influenza (HPAI): an emerging disease threat in North America. Ornithol Appl. Accessed January 2026.
- Li Q, Zhou L, Zhou M, et al. Comparative epidemiology of human infections with avian influenza A H7N9 and H5N1 viruses in China: a population-based study of laboratory-confirmed cases. Lancet. 2014;383(9932):1761-1769. doi:10.1016/S0140-6736(14)60101-3
- Writing Committee of the Second World Health Organization Consultation on Clinical Aspects of Human Infection with Avian Influenza A (H5N1) Virus. Avian influenza A (H5N1) infection in humans. N Engl J Med. 2008;358(3):261-273. doi:10.1056/NEJMra0707279
This lesson was last updated June 12, 2026